Improving Targeting of a Conditional Cash Transfer Program in Indonesia
- Men and boys
- Women and girls
- Social service delivery
- Cash transfers
Governments frequently struggle to ensure that social programs reach the people they intend to support. Researchers conducted a randomized evaluation with the Indonesian government that compared self-targeting to automatic screening in the context of a conditional cash transfer program. Requiring households to apply for a cash transfer program in Indonesia discouraged rich households from seeking out benefits and identified a relatively poorer group of beneficiaries.
Policy issue
Governments frequently struggle to ensure that social programs reach the people they intend to support. Correctly identifying households that are poor enough to qualify for a social program, or targeting, can be difficult if governments lack reliable income data to distinguish the eligible from ineligible. Without dependable targeting methods, policymakers risk incorrectly excluding poor households from social programs, incorrectly providing benefits to richer households, or both.
| Proxy Means Testing (PMT) |
| A PMT predicts consumption using households’responses to various questions, including: |
| Size of house |
| Roof material |
| Wall material |
| Motorbike ownership |
| Refrigerator ownership |
| Household head’s education |
| Household head’s occupation |
| Number of household members |
| Age and gender of household members |
As formal data on income is scarce in many countries, some governments employ proxy means tests (PMTs) to screen households for eligibility. PMTs predict income by collecting information about households’ assets. Since administering PMTs to all households is costly, many governments rely on administrative data to identify which households may qualify for the program and should receive the test. An alternative method to determine eligibility relies on governments to define requirements to receive benefits, such as applications or meetings with program administrators.
Since requirements can increase the time, effort, or monetary costs of qualifying, they might discourage the rich and disproportionately encourage the poor to seek out the program, a process called self-targeting. But these costs could also mean fewer poorer households apply overall. To test which method more accurately identifies poor households, researchers conducted a randomized evaluation with the Indonesian government that compared self-targeting to automatic screening in the context of a conditional cash transfer program.
Context of the evaluation
Indonesia’s Program Keluarga Harapan (PKH) aims to provide conditional cash transfers to the country’s poorest households. PKH beneficiaries receive between IDR 600,000 (US$67) and IDR 2.2 million (US$247) annually depending on family composition for up to six years. Households must meet certain requirements, including sending their children to school, attending pre- and post-natal check-ups, and completing vaccinations for children, to receive the quarterly transfer. To be eligible for PKH, a household must include a pregnant woman, a child under five, or children under 18 with less than nine years of schooling, and its per capita consumption must be less than 80 percent of their local district’s poverty line. Because consumption is not easy to observe, the Indonesian Government administers a proxy means test (PMT) to estimate it.

Details of the intervention
In 2011, the Indonesian Government expanded the geographic coverage of PKH to include new districts in Lampung, South Sumatra, and Central Java provinces. Researchers partnered with the Indonesian Central Bureau of Statistics (BPS) and Mitra Samya, a local NGO, to evaluate a new process for determining household eligibility. Researchers randomly assigned four hundred villages from two districts in each province to one of two targeting methods. Villages either followed the status quo procedure of automatic screening or the self-targeting method, which required households to apply to PKH.
Additionally, within self-targeting villages, researchers varied the distance to the registration sites. Half were randomly assigned to locate registration sites either close to the village, requiring households to travel zero to 0.8 kilometers on average, or far from the village, an average distance of about 1.2–3.1 kilometers. The difference in average travel distance between villages assigned to close and far registration sites was 1.6 kilometers.
To compare PKH beneficiaries to nonbeneficiaries in self-targeting and automatic screening villages, researchers surveyed households to measure consumption and assess experience with the targeting process and matched this information to BPS administrative data.
Targeting methods Automatic screening:Automatic screening did not require households to take any action to be considered for benefits. BPS and local officials first made a list of potential beneficiaries based on who received similar programs in the past or who local officials thought might be eligible. All households on the list were then administered a five-question screening at their homes and, if they passed the screening, the full PMT questionnaire. Households were eligible for PKH if their predicted consumption levels fell below each district’s cutoff. Self-targeting:Self-targeting required households to invest time and effort to be considered for PKH. Households needed to go to central registration sites to apply for benefits. Those who showed up to apply received the PMT interview at the registration site. To publicize sign-up, Mitra Samya hosted neighborhoodlevel meetings to explain the registration process, stressed that PKH was geared to the very poor, and shared information on where and when to apply. BPS visited households who passed the screening at the registration center to verify the information through another PMT, administered at home. Households were eligible for PKH if their predicted consumption levels fell below each district’s cutoff, just as in automatic screening. On average, the time and monetary costs of registering for PKH amounted to IDR 17,000 (US$1.91). By comparison, the average benefits from the program were approximately IDR 1.3 million (US$145.91) per year for six years.
Results and policy lessons
When households were required to apply for benefits, poorer households were more likely to apply than richer households.
Applicants were poorer than nonapplicants according to both measures assessed by the PMT, as well as other measures such as health, access to or use of services, and assistance from family or friends.
Overall, 38 percent of households in eligible villages applied to receive PKH. The likelihood that a household applied decreased as that household’s consumption increased. Among the very poorest households (i.e., those with expenditures in the bottom 5 percent), 61 percent applied to receive the program. Among the richest 5 percent of households, 10 percent of households sat for the preliminary asset interview.
PKH benefits reached more of the very poorest households in self-targeting villages.
The per capita consumption of beneficiaries in self-targeting villages was 18 percent lower than beneficiaries in automatic screening villages. Households with expenditures in the bottom 5 percent were more than twice as likely to receive benefits in self-targeting villages as in automatic screening villages. PKH awarded benefits to 16 percent of households with the lowest expenditures in self-targeting villages compared to 7 percent in automatic screening villages.
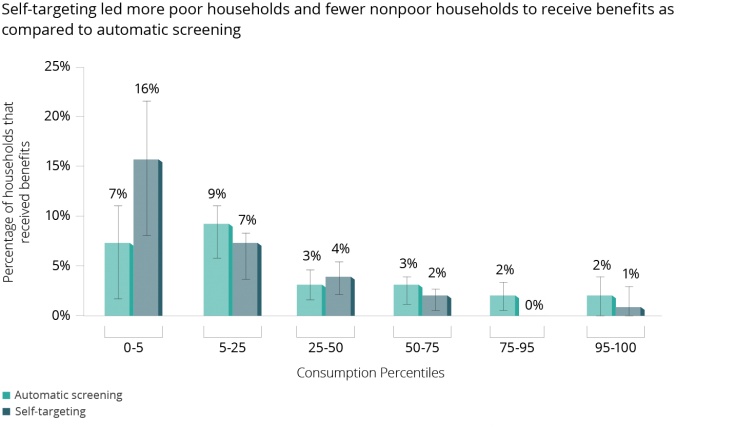
Self-targeting denied benefits to more nonpoor households relative to automatic screening, reducing the share of ineligible households that were incorrectly included.
The richest 50 percent of households, as measured by expenditures, were less than half as likely to receive benefits in self-targeting villages. One percent of these households received benefits in self-targeting villages, compared to 2.5 percent under automatic screening. This suggests that nonpoor households believed they had little chance of receiving benefits and consequently were unwilling to spend even a small amount of time and money to apply.
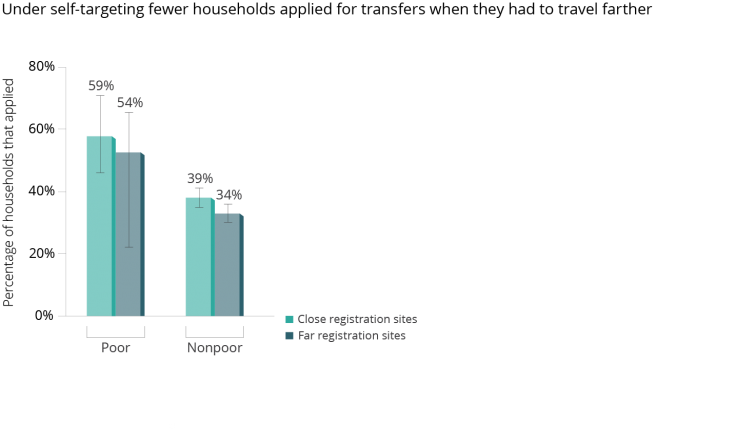
Increasing the distance to registration sites in self-targeting villages reduced the total number of applicants, but did not result in a higher share of eligible households within the applicant pool.
Increasing the distance to the registration site by 1.6 kilometers decreased application rates by 5.8 percentage points (13 percent). But the applicant pool in villages with farther registration sites, while smaller, included the same distribution of poor and nonpoor households as villages with close registration sites. In short, a small cost of applying led to better targeting than a larger application cost, which simply discouraged everyone.
Imposing a small cost to apply for a program can improve the process of awarding benefits by encouraging self-targeting.
Households in self-targeting villages spent roughly half a day visiting the central registration site at an average cost of IDR 17,000 (US$1.91), a small amount relative to PKH’s average annual benefits of IDR 1.3 million (US$145.91). Moreover, this process discouraged many nonpoor households from applying, as they may have perceived little or no chance of receiving benefits and were unwilling to spend even a small amount of time and money to apply.
Encouraging self-targeting by imposing an application cost might help programs serve more intended beneficiaries with fixed government resources.
In this case, self-targeting awarded benefits to poorer households than automatic screening. As such, researchers estimate that, for the same government budget, selftargeting could achieve a greater reduction in poverty.
Moreover, researchers predict that self-targeting would outperform universal screening, a hypothetical situation where every household would be given the PMT. In theory, determining the eligibility of all households, rather than first relying on census data to identify who should receive the test (as automatic screening does), might reduce the risk of excluding eligible households if the very poorest households do not appear in government data. However, universal screening would be very costly to implement. Projections suggest that self-targeting would select the very poorest households with equal success and would be less likely to award benefits to nonpoor households compared to universal screening.
While introducing a small cost improves targeting, marginally increasing those costs may not further improve targeting.
Applicants in villages who had to travel farther to apply were not any poorer on average than those in villages with closer registration sites. This suggests that keeping costs small might minimize the burden to the poor of applying for benefits while still encouraging self-selection.